After deadly spike, WA looks for advocates in pregnancy care
The story was originally published in Seattle Times with support from our 2022 Data Fellowship


Trinity Landrum holds her one-day-old son Messiah Divine Knight Providence at the postpartum unit at Providence Swedish First Hill. Landrum said having doula LaShaye Stanton-Phillips at her side during her C-section was a comfort and support. “Because of my previous experiences it’s hard for me to trust the system,” she said.
Erika Schultz / The Seattle Times
Tethered to IVs and fatigued with restless anticipation, Trinity Landrum distractedly nodded to the legion of scrubs scurrying in and out of her hospital room. A blood pressure cuff swelled on her left arm; a nearby monitor beeped indicating a dropping heart rate.
Instinctively, she rubbed her belly and the baby inside. Outside Providence Swedish Hospital First Hill, ambulance sirens cut through the quiet cold April night.
After 37 weeks of a healthy pregnancy, Landrum, 27, had frequent bouts of headaches and high blood pressure. They were symptoms of preeclampsia — the leading cause of death for Black mothers.
You could get really sick, her doctor warned, recommending an induction. She rattled off more severe risks: seizure, stroke, death.
As the labor-inducing drug Pitocin coursed through her veins, Landrum squeezed her partner’s hand, praying for a natural birth. But her baby was in distress. A cesarean section was imminent.
Realizing this, she broke into tears. Landrum knew the statistics.
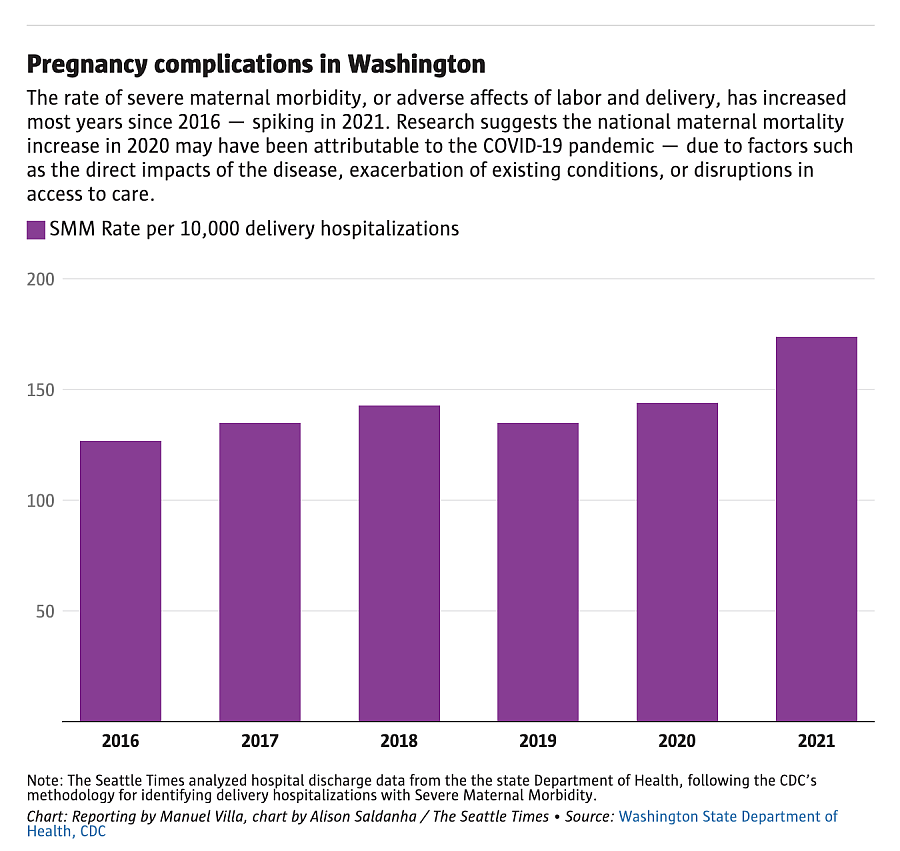
Black and Native people in Washington state, the majority of whom are on Medicaid, are three times and six times more likely, respectively, to die during pregnancy than white people. Overall, pregnancy-related deaths hit an all-time high in the state between 2018 and 2020, according to a new report from the state Department of Health, and are on the rise across the U.S.
Death is the extreme outcome. Pregnancy complications and illnesses affect many more people, especially from vulnerable communities. The health crisis is pushing health officials to prioritize access to culturally competent care to close racial gaps in care and improve outcomes.
Landrum tried to compose herself, but her meticulously prepared, low-intervention birth plan was unraveling. A soft voice interrupted her darkening thoughts: “Trinity, we prepared for this — you got this. You are amazing.”
It was LaShaye Stanton-Phillips, her doula, who has been a constant, reassuring presence throughout her pregnancy.

Doula LaShaye Stanton-Phillips worked with mother Trinity Landrum and her family at Providence Swedish First Hill. Stanton-Phillips says she wants mothers to know they are the most important person in the room. “I like to empower them and let them know, “This is a birthday party and you’re responsible for it,” she says. “We work for you. You’re not working for us.”
(Erika Schultz / The Seattle Times)
When Landrum was wheeled into the operating room, Stanton-Phillips, 40, was by her side. She held her hand and then set a Bluetooth speaker beneath her pillow.
Mary J. Blige’s soulful voice filled the sterile room. Landrum was ready.
At 4:09 on Easter morning, she safely delivered her rainbow baby, Messiah Divine Knight Providence.
While doulas like Stanton-Phillips do not provide medical care, they offer critical emotional, physical and educational support through pregnancy and after, advocating for families’ needs and rights within the hospital system.
The state Department of Health has proposed funding and training more doulas, as well as doctors, nurses, midwives and other health workers from vulnerable communities.

Doula LaShaye Stanton-Phillips, left, visits mother Trinity Landrum the day after she gave birth to her son Messiah Divine Knight Providence at the postpartum unit at Providence Swedish First Hill. “A lot of women would feel more comfortable and safe within their own birthing experience if they had access to a doula,” says Landrum.
(Erika Schultz / The Seattle Times)

Cam Providence, son Messiah Divine Knight Providence, 1-day-old, and Genesis Providence, 5, inside the postpartum unit at Providence Swedish First Hill in April.
(Erika Schultz / The Seattle Times)

Trinity Landrum breastfeeds her 1-day-old son Messiah Divine Knight Providence with the help of doula LaShaye Stanton-Phillips at Providence Swedish First Hill. “When you have someone that looks like you that works in the medical field, they understand what our struggle may be or some of the challenges that we might be experiencing,” says Landrum. She says a doula, like Stanton-Phillips, can advocate for mothers and make sure their voice is being heard.
(Erika Schultz / The Seattle Times)
“If there is a proven, evidence-based intervention that actually will address inequities in outcomes, I would put my money on doulas as number one,” said Beth Tinker, clinical nurse consultant for the Washington state Health Care Authority. “Number two would be midwives — especially midwives of color.”
A Cochrane review of studies suggests significant benefits to people who get support throughout pregnancy. For instance, continual support is tied to a 39% reduction in C-sections, shorter labor and a 10% drop in use of pain medications.
Doulas, Tinker said, are the most diverse health care profession and an immediate resource to tap into for better specialized perinatal care. Most others require an investment of time and money that could be prohibitive for people from communities facing the worst health outcomes.
A C-section five years ago and a miscarriage in 2021 left Landrum traumatized and distrustful of the health care system. Like so many Black mothers, she recalled regularly feeling dismissed and fighting to be heard.

Trinity Landrum works with doula LaShaye Stanton-Phillips during an appointment a few days before the birth of her son at Providence Swedish First Hill. “When I’m receiving my care, I want more additional feedback, perspectives, information and I felt like that was something that a doula could provide me,” says Landrum.
(Erika Schultz / The Seattle Times)
When she found out she was pregnant again, she chanced upon Providence Swedish Health’s new doula program and promptly signed up. The JUST Birth Network program, introduced in 2022, offers culturally affirming care for Black and Native families during a pregnancy through a dedicated network of childbirth cultural navigators, educators and birth and postpartum doulas.
“Having access to a familiar face, someone who looks like me, talks like me and has the necessary medical knowledge to navigate this system, transformed my experience,” Landrum said.

Trinity Landrum pats the back of her 1-day-old son Messiah Divine Knight Providence after feeding at Providence Swedish First Hill. Messiah was born on Easter.
(Erika Schultz / The Seattle Times)
Where she was first hesitant to ask questions, she now openly shared fears and concerns and decisively asked for explanations and alternative treatments. During hospital visits, she felt confident if she missed something, Stanton-Phillips would not. Together, they explored her options in every situation.
“Because of my doula, I was able to accept my birthing experience for what it was,” she said.

Vikki Compo plays with her grandson Michael Wallulatum, 2, outside the Ttáwaxt Birth Justice Center. The center is led by Jessica Houseman-Whitehawk, Leslie Swan, Tashina Nunez and Semone Dittentholer and supports families who live on and around the Yakama Nation Reservation.
(Erika Schultz / The Seattle Times)
“Felt like home”
Washington’s pregnancy-related death rate is slightly higher than the national average and more than twice the rate in any other highly developed countries such as Canada, France, Germany and Norway, according to latest data from the DOH.
Access to perinatal care in the state — key to preventing maternal morbidity and mortality — is similarly comparable to the national average, yet a closer look reveals a great divide between urban and rural areas.
Rural Washington reports a 40% higher rate of deaths during pregnancy or in a year after delivery, according to DOH. These geographic disparities worsen at the intersection of race, ethnicity and income.
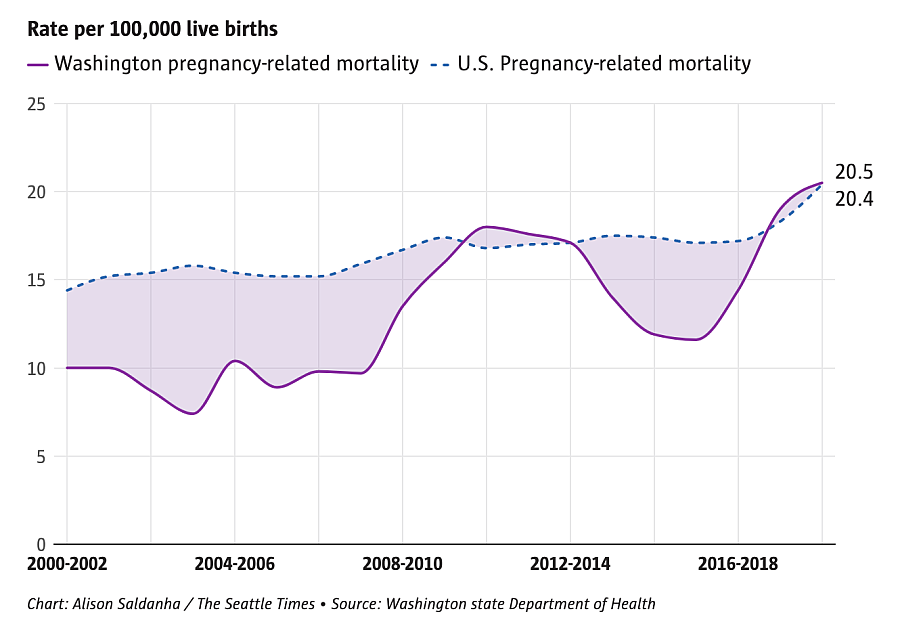
Chart: Alison Saldanha / The Seattle Times Source: Washington state Department of Health
Poor access and delays in care, inadequate health screenings, follow-up care, and discrimination are top contributing factors for Washington’s worsening state of maternal health, according to a DOH expert panel studying pregnancy-related deaths from 2014 to 2021.
Rates of C-section births in Washington and the U.S. are also alarmingly high compared to other nations, with the highest rates among Black mothers, according to a 2022 March of Dimes report.
While they are lifesaving in medically necessary situations, or a preference for some, it is still a major surgery with immediate and long-term risks for pregnant people. The report calls for a reduction in rates to improve outcomes.

Jessica Houseman-Whitehawk, executive director and founder of the Ttáwaxt Birth Justice Center, located on the Yakama Nation Reservation. Houseman-Whitehawk, a mother of three, is a member of the Winnebago tribe of Nebraska and of Santee Sioux descent.
(Erika Schultz / The Seattle Times)
American Indian and Alaskan Natives have the highest maternal and infant mortality rates in Washington state.
“Across the board, our statistics, our health outcomes show we have been left behind as the first people of this country,” said Jessica Houseman-Whitehawk, executive director and founder of the Indigenous women-led Ttáwaxt Birth Justice Center on the Yakama Nation Reservation.
Eleven years ago, after surveying women living in and around the reservation to gauge health care needs and wants, Houseman-Whitehawk, a member of the Winnebago tribe of Nebraska and of Santee Sioux descent, co-founded the center with Carmanita Pimms, the late executive director of Campbell Farm, a Presbyterian ministry mission near Wapato, Yakima County.

Birth justice advocate and manager Leslie Swan shows baby moccasins at the Ttáwaxt Birth Justice Center. Swan teaches classes on how to make the moccasins and gives out kits for mothers to make them at home.
(Erika Schultz / The Seattle Times)
The DOH and the community agree culturally inept health systems are failing Indigenous people, and solutions to improve outcomes must come from within. Bridging birth justice — a growing movement to protect the rights and choices of people giving birth — with ancestral knowledge on community healing and Western medicine, Ttáwaxt offers one such solution.
Sunlight poured into the center on an April afternoon as over half a dozen mothers, infants and toddlers filled the living room for a play group.
Houseman-Whitehawk and Leslie Swan host monthly Babes-n-Play to build community and connect families with the Nurse-Family Partnership. Nurses guide mothers on how to support each baby’s growth at the right stage of development.

Celeste Cantu, center, plays with her daughter Izabella Cantu, 1, while talking to Tori Wapsheli, right, and a group of mothers during a Babes-n-Play meetup at the Ttáwaxt Birth Justice Center. “What makes this work is that we are being who we are,” says Jessica Houseman-Whitehawk, executive director. “We are designing a new health care system and it does not erode who we are as Indigenous people. We have been fighting for sovereignty and autonomy for hundreds of years.”
(Erika Schultz / The Seattle Times)
Mothers and babies sat on a rug as Terel Cuevas, a registered NFP nurse, lifted toys out of a laundry basket for the children. “Increase her tummy time” she said to one mother, explaining how it helps the baby’s neck and trunk muscles.
Holding her 8-month-old as she waddled a few steps, Mercedes Andrews, 27, said she came to Ttáwaxt after attending classes at another birth center in the Tri-Cities area.
There, she felt self-conscious and afraid to ask for help. “When I came here, it immediately felt like home. I could ask a question and feel no hesitation or judgment.”

Jessica Houseman-Whitehawk, executive director and founder of the Ttáwaxt Birth Justice Center, left, talks with Tori Wapsheli during a Babes-n-Play meetup. “We are rebuilding our kinship and community centered around birth, family and providing excellent health care and other support that is needed in our community,” says Houseman-Whitehawk.
(Erika Schultz / The Seattle Times)
In the kitchen, Houseman-Whitehawk cooked green beans, bitterroot and coconut rice on the stove. A tray of baked salmon seasoned with herbs and spices sat on the counter next to a jug of cucumber and herb-infused water. Indigenous postpartum nutrition, she explained.
Today, Ttáwaxt has three doulas, two visiting nurses and a regularly visiting OB-GYN supporting comprehensive perinatal and women’s health on the reservation. The center is also connecting with other tribal communities across Washington to strengthen the network of focused Native care.

Herbal teas are stored at the Ttáwaxt Birth Justice Center, which was founded and is led by Native women on the Yakama Nation Reservation. The Ttáwaxt Birth Justice Center offers a variety of services, from pre- and postnatal support to doula services to plant medicine and cultural classes.
(Erika Schultz / The Seattle Times)
Ttáwaxt frequently leans on community elders to share valuable knowledge about culture for the next generation.
For Celeste Cantu, 30, who didn’t grow up on the reservation, that is critical.
“My mom didn’t teach me because she wasn’t taught much so I didn’t really know much,” she said. “But I can learn now and teach my daughter and pass down our traditional cultural teachings to her.”

Haylie Sullivan, left, holding Elijah, 3 months, and Rachel Farline, holding Griffin, 5 months, talk during a Baby and Me group, which offers support for local mothers and babies at the Columbia Birth Center in Richland.
(Erika Schultz / The Seattle Times)
Building trust
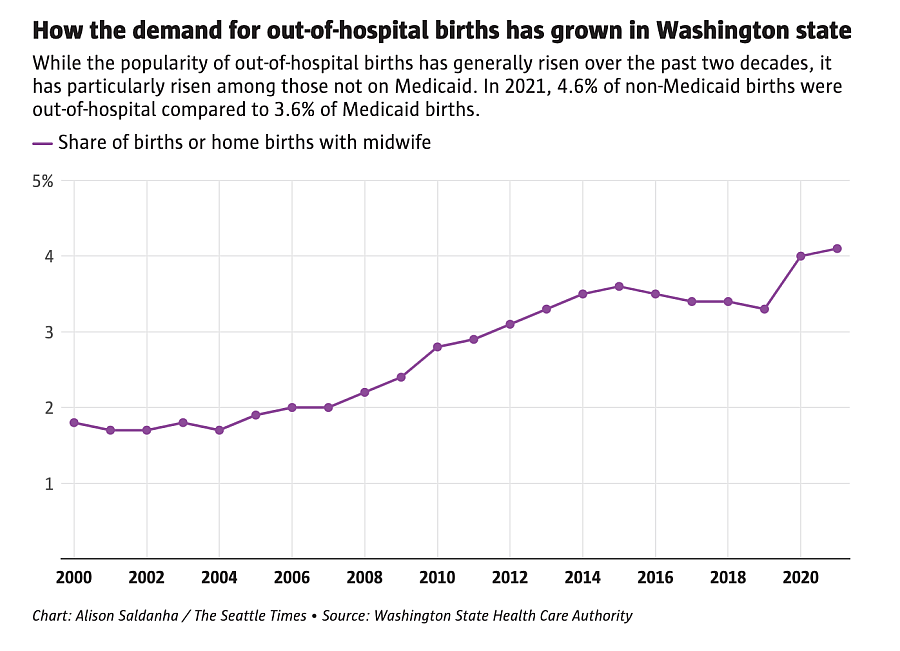
Acknowledging the trust health care providers can build outside hospital systems, the DOH expert panel endorses more out-of-hospital birthing care. This could also ease deficiencies in labor and delivery care in rural parts of the state, where these units have been among the first services cut as Washington hospitals face financial turmoil.
Currently, 24 of 39 Critical Access Hospitals in Washington, providing essential health services to rural, underserved communities, do not offer obstetric care, according to state DOH data.
In maternity health deserts across the state, it is a 34-mile drive, on average, to the nearest labor and delivery service. Often, people don’t have good transportation options to travel these distances and are forced to deliver in emergency departments. There are also fewer doulas and midwives operating in areas where hospitals have closed obstetric units.

Samantha Davidson and her son Shiloh Davidson, 9 months, are photographed at the corrals next to her home in Basin City, Franklin County, about 45 minutes north of the Tri-Cities. Davidson gave birth to four of her sons at hospitals, but decided to try the Columbia Birth Center in Richland, with her son Shiloh after it was difficult to get doctors appointments. She said birthing center felt more holistic and supportive supportive for her and her husband, allowed her children to come to appointments, and offered more choices and agency.
(Erika Schultz / The Seattle Times)
“There is definitely a concern among mothers in these areas of what happens if you don’t make it to the hospital? Like, do you deliver a baby in a car?” said Samantha Davidson, who lives in Basin City in Franklin County in Central Washington, and travels over 40 minutes to get to a hospital.
Last year, Davidson, 29, opted to deliver her fifth child at the Columbia Birth Center instead of the hospital next door. They won her trust when her midwife assured her she would come deliver the baby in a car if the situation arose.
“Instead of being like, ‘Hey, once you get here, you will be taken care of,’ it was very much like ‘We will take care of you, however you need,’ ” she said.
Most pregnancy-related deaths happen postpartum, indicating gaps in care after birth that doulas and midwives can bridge and better coordinate, experts say.
The extended time they spend with clients allows them to prescribe diet and supplemental care fitting their financial and cultural needs. They can be a key resource for identifying behavioral health conditions like postpartum depression and substance abuse — leading causes of pregnancy deaths in the state.

An altar with a photo of Carmanita Pimms, former executive director of The Campbell Farm and co-founder of the Ttáwaxt Birth Justice Center, is seen in Wapato, Yakima County
(Erika Schultz / The Seattle Times)
New mothers usually get a one-time postpartum checkup four to six weeks after giving birth, per the guidelines of the American College of Obstetricians and Gynecologists. Though these have since been updated to recommend more frequent care, several hospitals and clinics have yet to catch up.
“By six weeks, everything is hunky dory. It’s in between that they need the most care and attention,” said Olga Gadomskiy, a midwife with Sky Valley Midwifery serving Yakima, Benton, Franklin and Walla Walla counties.
Using the excuse of checking in on the baby, Gadomskiy also watches the mother closely to access her well-being, at least three times before the final six-week postpartum visit.

he names of babies born are displayed in the family room of the Columbia Birth Center in Richland.
(Erika Schultz / The Seattle Times)

Agricultural fields and farming equipment are seen at dusk near the Tri-Cities.
(Erika Schultz / The Seattle Times)
Certified solution?
Washington lawmakers passed legislation in 2022 to create a new health profession for birth doulas, which includes a process for state certification of doulas.
By becoming state-certified, they will be eligible for insurance reimbursement, broadening their reach to pregnant people in vulnerable communities, overrepresented in the Medicaid population and otherwise without means to afford this critical support, DOH said.
However it will still take a couple of years for doula care to be recognized as a covered benefit through Medicaid and other health insurance, Tinker said.
“It’s going to be a major funding ask from the Legislature because it’s reimbursing a whole new type of provider for a whole new set of services,” she said. “It takes a while, but we’re on the right trajectory.”
Still, several midwives surveyed by The Seattle Times say they struggle with insurance reimbursements despite credentialing.

Cynthia Flynn, a certified nurse midwife and advanced registered nurse practitioner, in one of the Columbia Birth Center’s birthing rooms in Richland, The center, which opened in spring of 2022, offers personalized care from midwives in a home-like environment. “People are driving further and further for care,” says Flynn. “It’s not just an issue in Washington state, it’s a national issue.”
(Erika Schultz / The Seattle Times)
“We are the only field in all of health care that doesn’t get paid for about a year for the work that we do,” said Cynthia Flynn, certified nurse midwife at the Columbia Birth Center in Richland.
They don’t bill someone until after a baby is born. And even then, it could take three months or longer for the reimbursement, she said.
Getting contracted with various insurance companies is also a barrier for many licensed midwives and birthing centers, who describe the process as tedious, time consuming and hardly worth the effort.
“There is a legitimate argument that insurance payments for their services need to be higher because of the amount of time spent with a mother,” said Paula Kett, a nurse research scientist at the Center for Health Workforce Studies at the University of Washington School of Medicine.
From the patient’s point of view, especially those on Medicaid, it limits what kind of support you have access to — an important piece to improving health results and inequities, she said.
As the state navigates new territory on credentialing doulas, many are wary the process could be another hurdle.

Tori Wapsheli holds 3-month-old Haylo Wolfe during a during a Babes-n-Play meetup at the Ttáwaxt Birth Justice Center. Wapsheli says she appreciates the support and help from the center.
(Erika Schultz / The Seattle Times)
“Sense of sisterhood”
Back at the Ttáwaxt play group, Houseman-Whitehawk fixed a plate for Shawnita Matta, 27. Houseman-Whitehawk took her 8-month-old daughter so the young mother could eat.
Matta is one of two doulas currently in training to join the birth justice center. Their ultimate goal is to build a full-fledged Indigenous-led and operated site on the reservation with all other cultural services.
“We’re learning from Ttáwaxt how to take care of ourselves and use natural medicines to heal our bodies. I feel like I’ve been able to recover faster from this birth because of their support,” Matta said.
Grateful for the “sense of sisterhood,” sharing this knowledge with others is a privilege, she said.
“We hope to have more women from our community serve our community so we can ensure the next generation continues — as life givers heal and become stronger, all of our community heals,” said Houseman-Whitehawk, as baby Dawn gurgled in her lap.